By Luiz Cláudio S Ferreira (DiveOps Nr 20)
The concept of diving gradients is directly related to the physiology of decompression and mathematical models that seek to predict the absorption and elimination of inert gases. From the first studies on decompression to the current models, gradients have been essential in the formulation of tables and strategies to minimize decompressive disease (DD).
The idea of pressure gradients arose with Paul Bert (1878) and John Scott Haldane (1908), who established the basis for dissolutive models. Haldane introduced the concept of half-life compartments and the supersaturation factor of 2:1. Robert Workman (1965) improved this approach by developing gradient factors (GF), a concept expanded by Eric Baker (1999) for more precise adjustments in technical diving computing.
Current decompression models include dissolutive, such as Buhlmann ZH-L16, bubble algorithm such as RGBM and VPM, and hybrids such as VPM-B and ZH-L16 with GF. Dissolutive models assume uniform elimination of gases, while bubble models incorporate microbubble growth control and adjustments according to the diver's previous exposure.
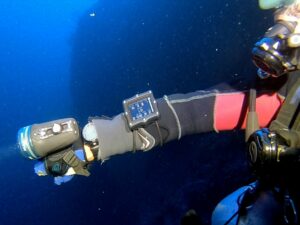
The application of gradients varies according to the diving profile and the specific conditions of the operation. In recreational dives (50 m), a more conservative adjustment, such as GF 30/70, optimizes safety without exceedingly prolonging the stops. In case of dives withrebreather(CCR), oxygen toxicity management and CO2 elimination efficiency may require specific adjustments in gradients. In deep dives (>100 m), the choice between GF 20/85 or a more open factor, such as 35/80 [Photo 1], depends on factors such as time planned in the background, gas logistics and external support, as well as the control of exposure to hostile environments. The decision on the appropriate gradient should always consider the need for balance between safety and efficiency, adapting to the physiological and operational demands of each dive, as well as the diver's own experience.
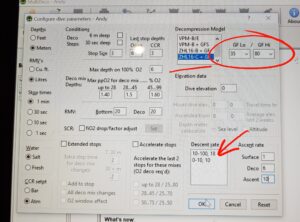
Photo 1
The concept of gradient factors can be seen in a graph that illustrates the relationship between the pressure of inert gases in the tissue compartments and the ambient pressure along the ascension. As shown in the figure, the high gradient factor (example: GF 30/80) directly influences the decompression starting point, allowing adjustments according to the diving profile. The M-value line represents the safe theoretical limit for the elimination of inert gases, while the ambient pressure line demonstrates the variation of pressure during the rise. The choice of more conservative FGs increases the safety margin by limiting the release rate of dissolved gases, reducing the risk of decompressive disease. Thus, the correct application of these factors enables a balance between efficiency and safety in decompression, as discussed in the strategies presented [Photo 2].
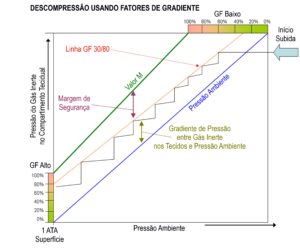
Photo 2
The choice of the decompression model, therefore, directly influences the applicability of the gradient. Dissolutive models tend to be more predictable for recreational and technical dives, while bubble models offer greater efficiency for deep and prolonged dives. In RGBM, for example, the microbubble plays a key role in adjusting decompression, while in ZH-L16 tissue saturation is the main factor. Hybrid models balance these approaches, allowing for more flexible climbing profiles.
The basic formula for determining the tolerable pressure of a tissue before controlled gas release is: Models such as RGBM add corrections for the presence of microbubbles, while ZH-L16 uses fixed compartments to predict saturation and elimination of gases. In deep dives withrebreather, efficiency of thescrubberand oxygen consumption rate also directly influence the application of gradients.
The choice between dissolutive and bubble models should consider depth, type of respiratory mixture and gas elimination rate. In use ofrebreathers, adjustments need to avoid hyperoxia. In multiple successive dive profiles, hybrid models can be more effective when considering gas accumulation over several exposures.
However, there are still relevant scientific gaps, such as the experimental comparison between different decompression models in deep dives, the impact of hypercapnia on the elimination of gases and adjustments in gradient factors, and the development of hybrid algorithms that combine the best aspects of each model. Research on probabilistic models of decompression and customization of algorithms based on individual physiology are promising.
In summary, gradients are essential in decompression planning, and the choice between dissolutive and bubble models should consider the diving profile and additional safety required. In-depth knowledge and correct application of these parameters are essential to ensure the safety of the diver, especially in extreme dives, where small variations can mean high risks. The domain of gradient factors allows the development of more efficient and adaptable strategies to different conditions, minimizing physiological risks and optimizing the efficiency of decompression. For technical divers, understanding and applying these principles not only increases safety, but also expands the possibilities of exploration in challenging underwater environments.

Author
Luiz Cláudio da Silva Ferreira
CMAS Instructor #M3/10/00001
PADI Tec TRIMIX/DSAT Instructor #297219
DAN Instructor #14249
#007.615.457-27