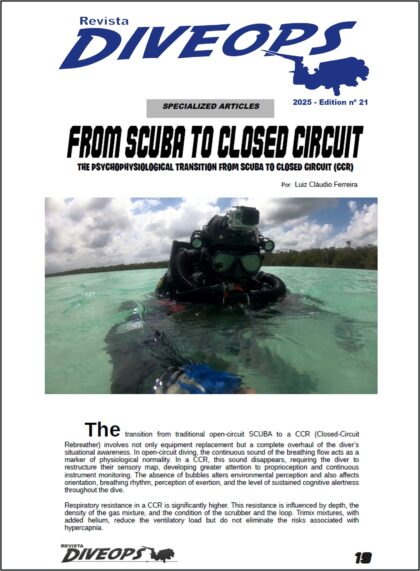
By Luiz Cláudio S Ferreira (DiveOps Nr 21)
The migration from the traditional SCUBA to the CCR involves not only the replacement of equipment, but the integral reformulation of the situational perception of the diver. In the open circuit, continuous noise of the respiratory flow acts as a marker of physiological normality. In CCR, this sound disappears, requiring the diver to restructure his sensory map, developing greater attention to proprioception and continuous reading of instruments. The absence of bubbles alters environmental perception and also impacts on the sense of orientation, respiratory rhythm, perceived effort and the degree of cognitive alertness sustained throughout immersion.

Opening – Source AlertDiver DAN
Respiratory resistance in CCR is significantly higher. This resistance is influenced by the depth, density of the gas mixture and the state of scrubber and loop. Trimix mixtures, with helium addition, attenuate the ventilatory load, but do not eliminate the risks associated with hypercapnia. The subjective perception of safety is reduced by the absence of auditory signals, forcing the diver to continuously monitor the PPO2 variation, sensor performance and respiratory system integrity. This requires mastery of ventilation itself under effort, constant mental discipline and ability to recognize early subtle signs of respiratory impairment before evolving to relevant physiological events.
The transition causes psychological discomfort even in experienced divers. The absence of family sensory landmarks from the SCUBA triggers adaptive anxiety, which may progress to decompensation if it is not adequately addressed. Conscious breathing techniques, attentional focus and load simulations help condition the emotional response. Trust built on years of conventional diving should be replaced by a new self-confidence based on technical doctrine, domain of complex systems [Fig 2] and assimilation of operational risks characteristic of the closed circuit.

Fig. 2 – Author Source
In CCR, surveillance needs to be constant. Scrubber failures, unscattered sensors and PPO2 off setpoint do not produce immediate sound alerts. The diver should be able to anticipate operational deviations based on frequent reading of critical parameters and perception of subtle respiratory variations. This requires cognitive discipline, operational memorization of contingencies and assimilation of typical circuit failures. Breath management becomes deliberate, not more instinctive.
In addition to the technical domain, the CCR diver needs to integrate advanced cognitive skills such as prolonged focus maintenance, silent failure management and dynamic physiological data-based decision-making. Response protocols should be internalized, and the use of a mental or physical checklist should be institutionalized in the immersion routine.
The most recent didactic approach adopted by schools proposes that the fundamentals of CCR be trained in modular and isolated stages, before the complete integration of the system in depth. This model reduces the initial cognitive overload and allows the student to gradually build a conscious relationship with the main elements of the circuit. — as the reading of PPO2, the verification of valves and the interpretation of respiratory loop dynamics. Training based on operational microcompetences creates a solid basis for critical decisions, establishing response patterns that can be automated without compromising subjective surveillance [Fig 3].

Fig 3 – InDepthMag Source
Advanced training should include simulated scenarios with PPO2 failure, sudden increase in respiratory density, and training to identify early-stage hypercapnia. The ability to maintain psychophysical stability under these conditions defines safety in extreme environments. The CCR extends time and depth limits, but requires constant technical surveillance and a new level of underwater self-management. Each decision must be made based on critical reading of parameters and constant ventilatory self-consciousness, incorporating the domain of respiratory physiology as an inseparable part of the operational conduct.
- OPERATIONAL CONCLUSION
The transition to the CCR represents an operational paradigm shift. Although it offers advantages such as greater autonomy, hydrodynamic profile and control of the respiratory mixture, it imposes a new psychophysiological and cognitive load on the diver [Fig 4]. The success of this migration depends on the integration between technical knowledge, real load training, emotional domain and full respiratory awareness. Training for CCR should incorporate realistic simulations, structured doctrine and progressive adaptation to operational silence, so that the diver learns to perceive risks not by obvious external signals, but by internal reading of the physiological response itself. The full understanding of this transition implies not only changing the respiratory technique, but adopting a new logic of internal command and psychophysiological supervision. It is about operating in an environment where the absence of noise may represent not tranquility, but a dangerous silence. The safety in CCR is not in the apparent comfort, but in the mental and operational structure that the diver builds before each immersion.

Fig 4 – Author Source
Author
Luiz Cláudio da Silva Ferreira
CMAS Instructor #M3/10/00001
PADI Tec TRIMIX/DSAT Instructor #297219
DAN Instructor #14249
#007.615.457-27