By Luiz Cláudio S Ferreira (DecoStop Nr 65)

Modern technical diving was born from the need to understand and control the physiological response of the human body to prolonged exposure to pressure. The scientific basis that supports it is a combination of empirical observation, controlled experimentation, and mathematical formulation. However, technological advancement—which brought sophisticated computers, software, and algorithms—also generated an unintended consequence: the belief that safety would be guaranteed by simply adhering to a specific decompression model.
Over the past few decades, the debate between dissolved models, based on Albert Bühlmann (1984), and bubble models, such as the Varying Permeability Model (VPM) and the Reduced Gradient Bubble Model (RGBM), proposed by Bruce Wienke (1999, 2008), has evolved beyond technique, becoming an almost ideological topic within the technical diving community.
This article proposes to critically analyze these models under three dimensions: scientific foundation, empirical verification, and practical interpretation. The examination is conducted based on experimental studies — such as the Navy Experimental Diving Unit (NEDU, 2011) report — and scientific reviews by Mitchell and Doolette (2013, 2020), complemented by analyses from the Divers Alert Network (DAN, 2023) and the technical recommendations of CMAS (2021). In addition, the contribution of John Chatterton (2004) is mentioned, whose operational experience illustrates the empirical phase of deep diving before algorithmic standardization.
The guiding question is simple: what do we really know — in a verifiable way — about the effectiveness of the decompression models we use?
Fundamentals of Dissolved Models: Bühlmann’s Legacy
The origin of decompression algorithms dates back to John Scott Haldane, who, in 1908, conceived the idea that the body could be divided into tissue compartments, each with a saturation and desaturation half-life of inert gases. Decades later, Albert A. Bühlmann, at the Zurich Hospital, expanded on this logic, refining the maximum tolerable pressure parameters for nitrogen and helium. His work, Decompression-Decompression Sickness (1984), consolidated the basis of what we now know as the ZH-L16 model, widely implemented in computers and planning software.
The model assumes that each tissue compartment absorbs and releases inert gas according to exponential equations, until equilibrium is reached. The risk of decompression sickness is controlled by limiting the permitted supersaturation — represented by the M values.
Bühlmann obtained his data through experiments in a hyperbaric chamber, monitoring volunteers undergoing simulated dives. By recording symptoms and empirically adjusting the saturation curves, he created a system that translates the observed experience into mathematical calculation. The accuracy, therefore, derives from applied empiricism, and not from a perfect physiological model.
In modern computers, the introduction of gradient factors (GFs) allows for modulating the tolerance to supersaturation: smaller values (such as 30/70) make the profile more conservative, while larger values (85/85) reduce the total time, accepting greater risk. This flexibility is a direct reflection of uncertainty: the diver chooses how close they want to get to the experimentally tested limits.

Figure 1 – Situation of tissue compartments at the end of decompression, when the upper gradient factor (GF High) reaches 70%, limiting residual supersaturation. Source: Suunto – Algorithm Settings, 2025
According to Mitchell and Doolette (2013), this plasticity reveals the essential character of the Bühlmann model: it is descriptive, not predictive. It serves to organize the experience of thousands of observed dives, but not to fully explain the complex interaction between gases, tissues, and microbubbles.
Bubble Models: Wienke’s Conceptual Revolution
In the 1990s, the increasing sophistication of mixtures and the advancement of trimix operations stimulated the emergence of models focused on bubble dynamics. Bruce Wienke formulated the RGBM (Reduced Gradient Bubble Model), derived from previous concepts of the Varying Permeability Model (VPM).
These models start from a different hypothesis: that gaseous micronuclei are present in the human body even in equilibrium, and that, by reducing the pressure, these nuclei can grow and generate clinically relevant bubbles. The strategy, then, would be to maintain higher ambient pressures for longer in the initial phases of ascent, delaying the expansion of the bubbles. This translates to deeper stops — so-called deep stops.
VPM and RGBM incorporate formulas that limit the critical growth of bubbles as a function of maximum depth and exposure history. The goal is to distribute decompression time more evenly, smoothing the pressure gradient between compartments.
This approach found strong support among technical divers, partly due to intuitive logic: if bubbles appear with the rapid increase in supersaturation, stopping earlier and for longer would seem prudent. However, subsequent empirical evidence has shown that this assumption is not always confirmed in practice.
The Role of Empiricism: Lessons from Experimental Evidence
The discussion about decompression only makes sense when confronted with observable data. Empiricism is the basis that validates — or corrects — the theory.
The NEDU 11-06 report (Doolette & Gerth, 2011) evaluated simulated dives with profiles containing deep stops compared to profiles without time redistribution. The result was unequivocal: dives with deeper stops showed a higher incidence of decompression sickness. The finding contradicted theoretical expectations and demonstrated that prolonging time at depth can compromise the efficiency of gas elimination in slow-moving tissues.
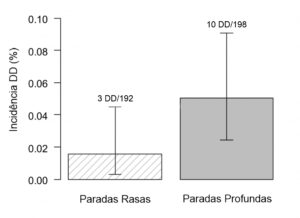
Fig 2 – Comparative graph of DD incidence between airfoil profiles with shallow stops versus airfoil profiles with deep stops, referenced in the 2011 Navy Experimental Diving Unit (NEDU) study. Source: CARUANA, J., 2018.
A 2011 study by the Navy Experimental Diving Unit (NEDU). Source: CARUANA, J., 2018.
In parallel, surveys by the Divers Alert Network (DAN, 2023) and DAN Europe (2022) analyzed tens of thousands of recreational and technical dives. The conclusions indicate that DCS is multifactorial: variables such as physical exertion, temperature, age, diving history, and individual anatomical conditions (e.g., presence of patent foramen ovale) have comparable weight to the ascent profile.
The studies by Mitchell and Doolette (2020) reinforce this view, arguing that deterministic models fail to encompass the biological complexity involved. In a review published in Comprehensive Physiology, the authors suggest that algorithms should be understood as risk management tools, not as safety guarantees.
Similarly, the American Academy of Underwater Sciences has demonstrated, in analyses of scientific diving, that the low accident rate is strongly associated with operational discipline — rigorous planning, effort control, and adherence to protocols — regardless of the mathematical model used.
In short: the data show that the success of decompression depends less on the algorithm and more on the consistency of human behavior under the protocol.
Dogma, Tradition, and Identity in Technical Diving
Among technical divers, the choice of a model has often become a mark of identity. Certain schools defend VPM or RGBM as symbols of an operational philosophy, while others remain faithful to Bühlmann with specific gradient factors. This segmentation is reminiscent of the formation of “lineages” — where the method is inherited more by culture than by scientific proof.

Fig 3 – Team Brazil in technical diving (OC) during an underwater operation on the Andrea Doria in 2016. Source: Autos, 2016.

Limitations of Current Models and Perspectives on Evolution
The limitations of current models are widely recognized by the scientific community. Recent physiological studies, such as those by Mitchell and Doolette (2020), show that the individual response to decompression is affected by factors that escape the mathematical scope: cardiovascular anatomy, inflammatory status, hydration, microcirculation, and silent microbubbles.
As a result, institutions such as DAN Europe, through the Diving Safety Laboratory (2022), have been compiling probabilistic databases with hundreds of thousands of real-world profiles. The goal is to replace binary reasoning (“inside” or “outside” the curve) with statistical risk estimates. This probabilistic approach—similar to those used in aviation medicine—allows for the consideration of individual variations and the generation of dynamic, personalized decompression models.
These advances point to a future where decompression will be increasingly adaptive. Instead of fixed profiles, we could have algorithms that incorporate real-time physiological data from the diver, such as heart rate, body temperature, and gas consumption.
Until this becomes a reality, the literature suggests a cautious approach: the technical diver should understand the model they are using, know the evidence that supports it, and adjust their behavior according to the actual operating conditions.
Conclusion
Decompression models are tools based on controlled empiricism, not systems of absolute truth. The Bühlmann ZH-L16 remains the most solid pillar, the result of decades of reproducible and widely validated experiments. Bubble models, such as VPM and RGBM, have made important conceptual contributions—especially in attempting to describe the role of micronuclei—but their practical performance has not confirmed the expected advantage.
The most robust evidence, such as the NEDU study (2011) and the reviews by DAN (2023) and Mitchell and Doolette (2020), converges on the same conclusion: the effectiveness of decompression depends less on the algorithm and more on operational discipline. Empiricism remains the basis of safety, and tradition only has value when aligned with evidence.
CMAS (2021) reinforces this view institutionally, recommending that profile adjustments should always be based on observational data and controlled reviews. This convergence between practice and science signals a maturation in technical decompression: overcoming blind faith in numerical models in favor of a culture of critical analysis.

Fig 5 – Hyperbaric chamber used for decompression experiments and physiological observation. Source: NASA / Wikimedia Commons, 2022.
On a philosophical level, the technical diver must recognize that every equation carries uncertainty. True mastery lies not in choosing between Bühlmann, VPM, or RGBM, but in understanding how each was constructed, tested, and limited.
Ultimately, safe decompression is an exercise in respect for history and evidence—from the empiricism of pioneers like Chatterton to the analytical sophistication of modern institutions. It is in this synthesis between experience and method that technical diving finds its contemporary identity: a field in constant revision, where science does not eliminate risk, but understands it in order to better manage it.
Bibliographic references (ABNT NBR 6023:2018 – complete and revised version)
BÜHLMANN, Albert A. Decompression-Decompression Sickness. Berlin: Springer-Verlag, 1984.
CHATTERTON, John; TALTY, John. Shadow Divers: The True Adventure of Two Americans Who Risked Everything to Solve One of the Last Mysteries of World War II. New York: Random House, 2004.
CONFÉDÉRATION MONDIALE DES ACTIVITÉS SUBAQUATIQUES (CMAS). Technical Committee Recommendations on Deep Stops and Decompression Practices. Rome: CMAS, 2021. Available at: https://www.cmas.org/. Accessed on: 11 Nov. 2025.
DIVERS ALERT NETWORK (DAN). Annual Diving Report 2022–2023: A report on diving incidents, injuries, and fatalities. Durham, NC: Divers Alert Network, 2023. Available at: https://dan.org. Accessed on: 11 Nov. 2025.
DIVERS ALERT NETWORK EUROPE (DAN Europe). Diving Safety Laboratory: Research and Statistics on Diving Profiles and Decompression Illness. 2022. Available at: https://www.daneurope.org/. Accessed on: November 11, 2025.
DOOLETTE, David J.; GERTH, Wayne A. Evaluation of Deep Stops for Air Decompression Dives. Panama City: Navy Experimental Diving Unit (NEDU), 2011. (NEDU Report 11-06). Available at: https://apps.dtic.mil/sti/pdfs/ADA552155.pdf. Accessed on: November 11, 2025.
DOOLETTE, David J.; MITCHELL, Simon J. Deep stops: does the evidence support the practice? Undersea and Hyperbaric Medicine, v. 40, n. 5, p. 445–457, 2013. DOI: 10.22462/05.06.2013.1.
HILLS, Brian A. A Thermodynamic and Kinetic Approach to Decompression Sickness. Undersea Biomedical Research, vol. 3, no. 3, p. 237–247, 1976.
MITCHELL, Simon J.; DOOLETTE, David J. Physiological and practical aspects of decompression stress: a review. Diving and Hyperbaric Medicine, vol. 43, n. 2, p. 68–76, 2013. DOI: 10.28920/dhm43.2.68-76.
MITCHELL, Simon J.; DOOLETTE, David J. Hyperbaric conditions, gas exchange, and decompression illness. Comprehensive Physiology, vol. 10, no. 3, p. 1105–1159, 2020. DOI: 10.1002/cphy.c190041.
WIENKE, Bruce R. Reduced Gradient Bubble Model (RGBM) and Deep Stop Implications. Technical Diving International (TDI) Proceedings, 1999. Available at: https://www.tdisdi.com/. Accessed on: 11 Nov. 2025.
WIENKE, Bruce R. Basic Decompression Theory and Application. 3rd ed. Flagstaff: Best Publishing, 2008.